Dr. Nik Tehrani
39270 Paseo Padre PKWY, Suite 424
Fremont, CA 94538
Phone: 510.676.5606 Fax: 510.550.4456 Email: nik@niktehrani.com
Abstract The Universal Declaration of Human Rights, an international human rights law, requires governments to provide right-to-health systems. One solution for reaching patients in remote locations to avoid costs associated with transporting health workers, and the sheer numbers of patients, is a remote health monitoring device. Also, the increase in the occurrence of chronic disease in an aging population ages leads to immobility, increasing the need for remote health monitoring devices as well. Results of cardiac rhythm disorders such as “atrial fibrillation (AF), bradycardia, atrioventricular (AV) block and sudden cardiac death” (Thibault and Guerra, 2010, para. 2) can be remotely gathered using digital technologies, such as wireless biosensors, integrated with traditional medical data and made accessible to doctors. Dyno Sense Corporation has developed a fully integrated multi-scan health scanner using nine sensors to measure 33 different health metrics using a new device called Dyno that can monitor all the critical vitals (ECG, heart rate, blood oxygen, respiration rate, breathing efficiency, blood pressure change, body temperature, plus others in development) at home or in a remote area. The Dyno has been proven in clinical trials to successfully monitor health conditions.
Keywords: Digital, Health, Remote, Monitoring, Sensors, ECG, Blood Pressure
INTRODUCTION
Improvements in social conditions and medical care in the Western world, in addition to advances in “pharmacologic and interventional management of patients,” (Thibault and Guerra, 2010, para. 2) have led to a significant increase in human longevity, allowing people to survive up to 80 years and beyond, often resulting in added health problems attributed to advanced age (Thibault and Guerra, 2010). As the population ages, the occurrence of chronic disease increases, creating problems for the health care system
The Universal Declaration of Human Rights is an international human rights law that obliges governments to provide right-to-health systems (Backman, Hunt, Khosla, Jaramillo-Strouss, Fikre, Rumble, Vladescu, 2008). Remote health monitoring is a solution for certain groups of patients in remote locations, due to complications and costs of transporting health workers and the large quantity of patients requiring health care (Spinsante and Gambi, 2012). Remote health monitoring interaction of patients with chronical diseases that have not undergone a physician’s medical examination can be achieved using remote health monitoring devices. Such remote health monitoring systems can be tailored to address a wide range of needs, according with each patient’s conditions (Spinsante and Gambi, 2012).
Broadband will be key to “supporting health care delivery in America” (Continua, 2010, para. 5) in the future. “The National Broadband Plan drafted earlier this year by the Federal Communications Commission (FCC),” could save the health care industry “$700 billion over 15 to 20 years” (Rouse, 2014) through the implementation of “remote patient monitoring technology in conjunction with electronic health records (EHR)” (Rouse, 2014, para. 4).
HEART
Advancing age of the populace has led to an avalanche of cardiac rhythm disorders such as “atrial fibrillation (AF), bradycardia, atrioventricular (AV) block and sudden cardiac death” (Thibault and Guerra, 2010, para. 2).
Increased incidences of AF can be attributed not only to the aging of the population, but also to co-existing illnesses and the ability to detect “asymptomatic episodes” using the “diagnostic capabilities of pacemakers and defibrillators” (Thibault and Guerra, 2010, para. 3). Along with advancing age and incapacitating medical conditions come problems with mobility, s it has become necessary to collect information in a way that reduces patient necessity to visit a physician’s office (Thibault and Guerra, 2010).
Technology allows digital communication and wireless transmission of patient information to be “integrated into implantable devices” (Thibault and Guerra, 2010, para. 9), that require regular follow up anywhere between and one to four times annually to evaluate the patient’s medical condition and how the device is functioning (Thibault and Guerra, 2010). This has been a challenge for large medical facilities and for those in remote areas. Recent technological advances have helped to improve safety for both patients and devices, permitting information to be transmitted directly to the physician, eliminating the need for patients to travel (Thibault and Guerra).
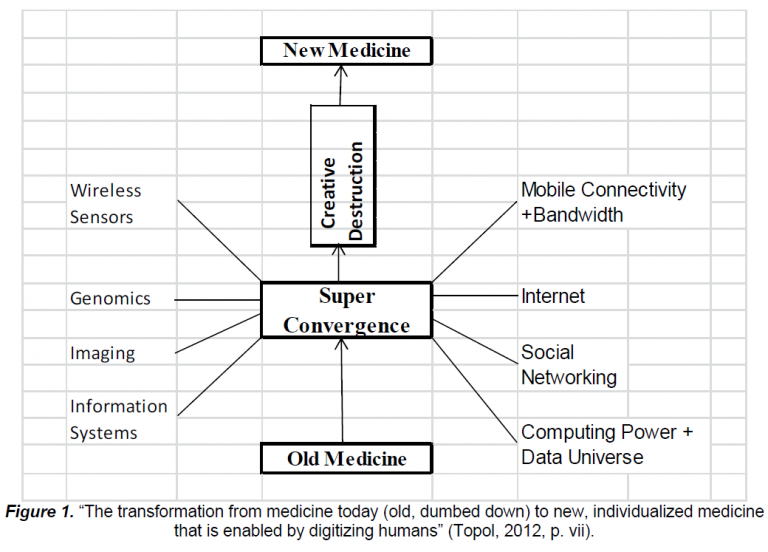
This digitizing of information about individuals could not have occurred if not for the maturation of world digital technologies, such as wireless biosensors integrated with traditional medical data which can be constantly updated (Topol , 2012).
Dyno Sense Corporation is a new company that has developed a fully integrated multi-scan health scanner using nine sensors to measure 33 different health metrics (Tehrani, 2015). The device, called Dyno, monitors all the critical vitals (ECG, heart rate, blood oxygen, respiration rate, breathing efficiency, blood pressure change, body temperature, plus others in development) remotely, essential for at home monitoring.
To validate and verify Dyno’s capabilities, DynoSense was invited to travel to China to run a clinical test on patients to compare results with standard hospital equipment. The China Trial was performed at China-Japan Friendship Hospital in August 2014 (China-Japan Friendship Hospital, 2014). Since the testing was to be done in a hospital setting, the trial sponsor was concerned about the Dyno device sanitization. Therefore, the device had to be modified to have the temperature probe removed. As a result, data from the China-Japan Friendship Hospital Trial was shown without the temperature data (China-Japan Friendship Hospital, 2014).
China-Japan Friendship Hospital tested and monitored 5 people using the Dyno, most of whom had heart conditions. The trial sponsor wanted to view, in particular, the ECG results of the heart problems in Dyno’s report. The doctors also compared the blood pressure measurement from hospital equipment and the measurement resulting from the Dyno test. The result was within the AAMI (Association for the Advancement of Medical Instrumentation) standard (China-Japan Friendship Hospital Trial, 2014).
DynoSense also conducted another test at an elderly care facility, SarahCare of Campbell, a leading provider of adult and elder day care services in the south Bay Area. Testing of the Dyno was performed over a four-day period, initially testing 14 people, and tracking 6 for the entire 4 days, with an average of 3 times per day per person. The purpose of this trial was to validate the Dyno results against commercially available gold standard equipment results. Out of the 6 people who were tracked, the Dyno reported that two women in their 70s had heart conditions, one with PVC and one with arrhythmia. DynoSense then used an FDA approved ECG device to verify the findings, which confirmed that the Dyno findings are valid (Sara-Care of Campbell, 2014).
HYPERTENSION AND REMOTE HEALTH MONITORING
A broad range of advanced communication methods are available for patient self-management of hypertension (Rothman, Wagner, 2003; Logan, McIssac, Tisler, Irvine, Saunder, Dunai…Cafazzo, 2007), such as home blood pressure (BP) monitoring devices and tele-management (Kaufman, Patel, Hilliman, Morin, Pevzner, Weinstock, Goland, Shea, and Starren, 2003; Logan et al, 2000). However, attempts to better BP control have not been very effective, due to tele-management systems requirements for wired connections, lack of expertise of elders using the Internet, the interference of physician work flow, and lack of personal communication between patient and physician.
The Logan et al. (2000) study concentrated on developing and “pilot-testing a mobile phone–based remote patient monitoring system to improve BP control of hypertensive patients with diabetes” (p. 946). The findings concluded that use of this system was highly accepted by patients, and physicians who received reliable data were able to reduce BP of diabetic patients with uncontrolled hypertension without disrupting their workflow. However, new solutions still need to be researched and developed (Garg, Adhikari, McDonald, Rosas-Arellano, Devereaux, Beyene, Sam, and Haynes, 2005; Logan et al., 2000)
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD)
A key goal of the respiratory community is the early detection of “Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD)” (Sund, Powell, Greenwood and Jarad, 2009, p. 1321) in COPD patients. AECOPD is a significant characteristic of the disease. Health status, such as quality of life, (Sund et al., 2009) often deteriorates due to recurrent pulmonary exacerbations (Sund, et al., 2009). AECOPD is often connected to an escalation in “symptoms, including cough, sputum volume/purulence and shortness of breath,” (Sund, et al., 2009, p. 1321) causing patients to seek medical help that often results in physicians intensifying treatment. If AECOPD goes untreated, the condition may gradually result in a drop in lung function. Early treatment of AECOPD is believed to result in shortened periods of symptoms and a chance to improve recovery; however, to manage AECOPD, patients must be diagnosed by their physicians at the early stages of symptoms. “Interventions aimed at delaying the progression of COPD and improve access to healthcare are considered high priority areas” (Sund, et al., 2009, p. 1328).
On August 28, 2014, Peking University First Hospital tested and monitored one person diagnosed with COPD who needed to wear an oxygen mask (Peking University First Hospital Trial, 2014). The patient had been admitted to the hospital multiple times in the past with the same problem. DynoSense Corporation was invited again to run the test. The doctor asked the patient to remove the oxygen mask for a moment to see how well the Dyno could track the patient’s condition.
The patient’s blood Oxygen measured by the hospital equipment dropped down to approximately 78% within a few minutes, and Dyno also tracked that rapid change in blood. A key vital that the doctor wanted to check was blood pressure. One interesting finding was that within minutes, multiple blood pressure measurements using a traditional cuff had large variations (14 mmHg variations in diastolic blood pressure when patient is in stable condition), while Dyno reported consistent blood pressure measurements across the different sessions (Peking University First Hospital Trial, 2014).
Dyno is a user friendly device that can be used as required with little effort and the information captured is securely stored. Dyno is the premier example of current advances in remote health monitoring devices. Physicians will be able to access real-time patient data, creating improved patient treatment (Tehrani, 2015).
REFERENCES
1. Backman, G., Hunt, P., Khosla, R., Jaramillo-Strouss, C., Fikre, B. M., Rumble, C., Vladescu, C. (2008). Health systems and the right to health: An assessment of 194 countries. The Lancet, 372(9655), 2047-85. Retrieved from http://search.proquest.com/docview/199013899?accountid=38235
2. China-Japan Friendship Hospital Trial (2014). DynoSense. San Jose, CA
3. Continua health alliance commends the FCC for health care provisions in its national broadband plan. (2010, Mar 17). Business Wire Retrieved from http://search.proquest.com/docview/443528849?accountid=38235
4. Garg AX, Adhikari NK, McDonald H, Rosas-Arellano MP, DevereauxPJ, Beyene J, Sam J, Haynes RB: Effects of computerized clinical systematic review. JAMA 2005;293:1223–1238.
5. Kaufman DR, Patel VL, Hilliman C, Morin PC, Pevzner J, Weinstock RS, Goland R, Shea S, Starren J: Usability in the real world: assessing medical information technologies in patients’ homes.
6. Logan, A. G., McIsaac, W. J., Tisler, A., Irvine, M. J., Saunders, A., Dunai, A., Cafazzo, J. A. (2007). Mobile phonebased remote patient monitoring system for management of hypertension in diabetic patients*. American Journal of Hypertension, 20(9), 942-8. doi:http://dx.doi.org/10.1016/j.amjhyper.2007.03.020
7. Peking University First Trial. (2014). DynoSense. San Jose, CA
8. Rothman AA, Wagner EH: Chronic illness management: what is the role of primary care? Ann Intern Med 2003;138:256 –261.
9. Rouse, M. (2014). Remote patient monitoring (RPM). Retrieved from http://searchhealthit.techtarget.com/definition/remote-patient-monitoring-RPM
10. Sara-Care of Campbell. (2014). DynoSense. San Jose, CA
11. Spinsante, S., & Gambi, E. (2012). Remote health monitoring for elderly through interactive television. Biomedical Engineering Online, 11, 54. doi:http://dx.doi.org/10.1186/1475-925X-11-54 12. Sund, Z. M., Powell, T., Greenwood, R., & Jarad, N. A. (2009). Remote daily real-time monitoring in patients with COPD – A feasibility study using a novel device. Respiratory Medicine, 103(9), 1320-8. doi:http://dx.doi.org/10.1016/j.rmed.2009.03.017
13. Tehrani, N. (2015). Taking control of health care Zenith international journal of multidisciplinary research. ISSN 2231- 5780
14. Thibault, B., & Guerra, P. G. (2010). Implanted cardiac devices with remote monitoring capacity: “it’s like having a physician follow me on a daily basis”. Expert review of cardiovascular therapy, 8(5), 617-9. doi:http://dx.doi.org/10.1586/erc.10.393.
15. Topol, E. J. (2012). The creative destruction of medicine: How the digital revolution will create better health care. New York: Basic Books.
Error: Contact form not found.